But anyways, the reason why I ask.
The NEC from the 70s had an allowance for a life support branch in addition to the critical branch- and the fact a fair share of pre 80s hospitals actually had a dedicated life support branch in conjunction with a separate critical branch.
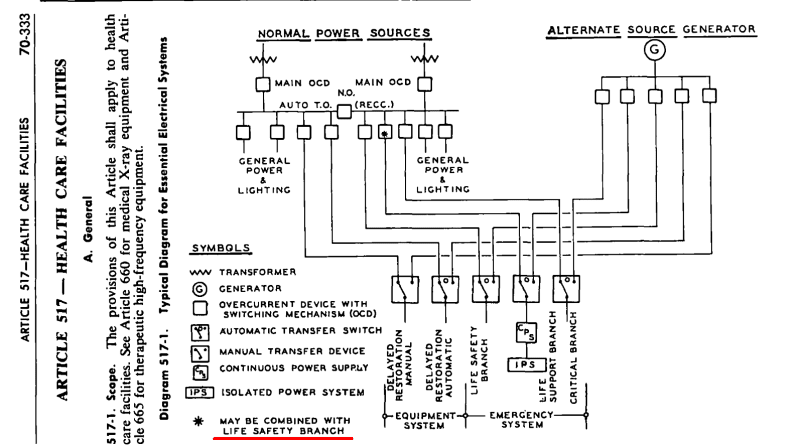
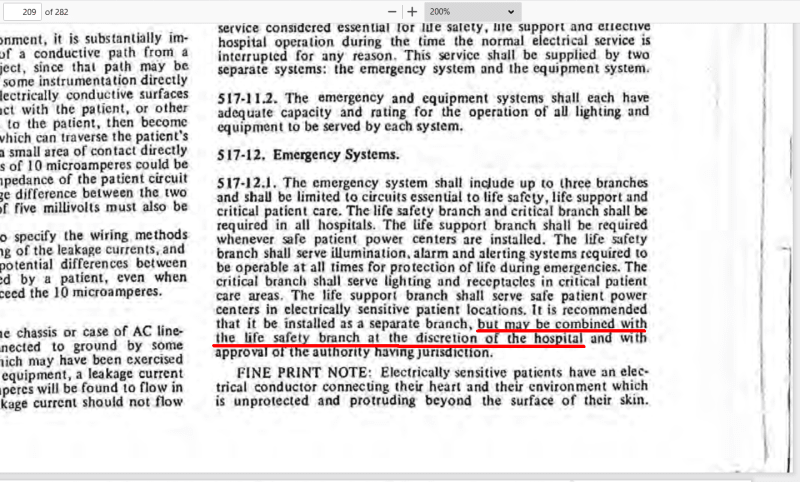
From the 1971 NEC:
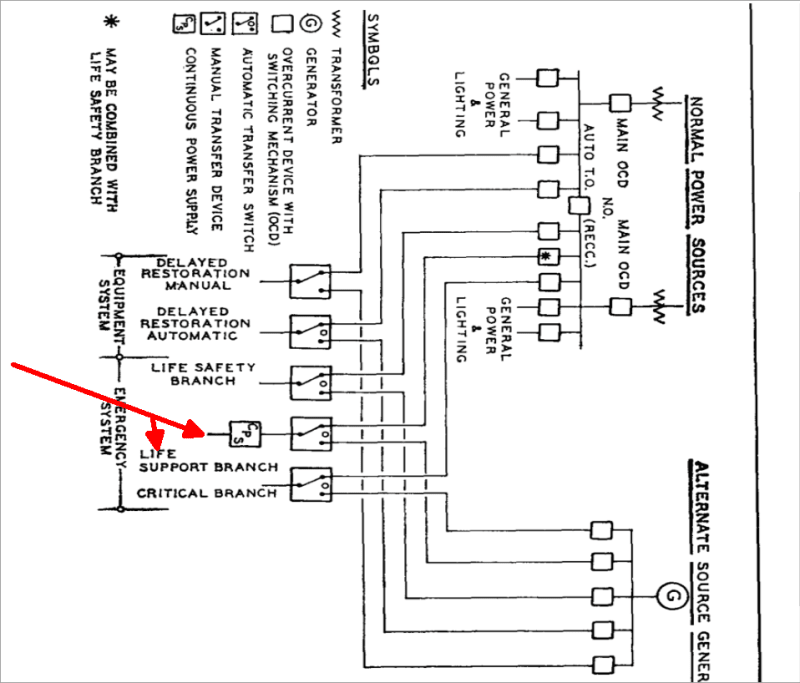
Graphic in the ROPs:
It is interesting to note that the CMPs originally agreed that the life support branch could be combined with the life safety branch if they were not separate.
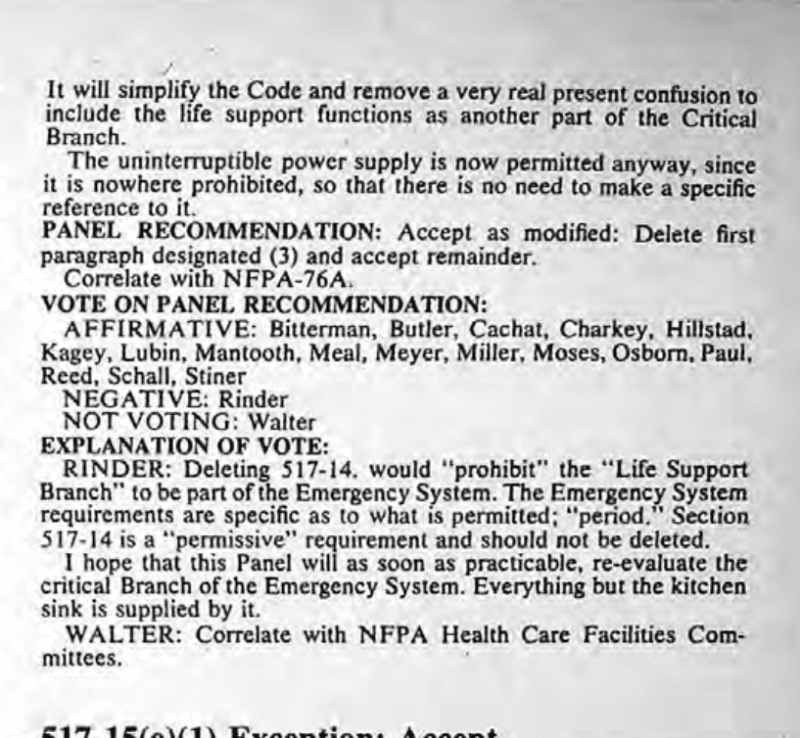
1971 ROP:
The life support branch was originally intended to receive the same fire protection and priority as the life safety branch which was (and still mostly is today) required to meet the requirements of article 700.
Latter on the CMPs changed their minds that the life support branch could be combined with critical branch instead of the life safety branch.
For the 1978 NEC a proposal was sent in to delete the concept of a life support branch:
Accepting the proposal was a fantastic impulse without any thought and hare-brained to be frank.
It took away the concept of a protected high priority branch that not only should/would have followed article 700 but also the greater probability of getting rid of the half and half approach in ORs and ICUs during design.
Hospitals work on the concept of compartmentalization, isolation and segregation to deal with fires. Evacuation of a whole hospital building is not possible or practical.
The requirements of 700 force the life safety branch to be protected from fire and in separate electrical rooms segregated from all the other branches in a hospital.
Yet the critical branch and normal branch are often in the same room without any fire protection be it in the shafts, interstitials, ceilings, partitions, walls, ect.
This wholly contradicts the compartmentalization approach to hospitals.
How the NFPA doesn't see this is beyond me, unless people incapable of self preservation (from being ill or different) are seen as lesser priority than those who are able bodied- which is not out of the realm of possible given history...
Hospitals outside of North America have a dedicated, protected life support branch in addition to a normal and critical branch.
North American hospitals for the last 50 years have been designed and built missing a life support branch.