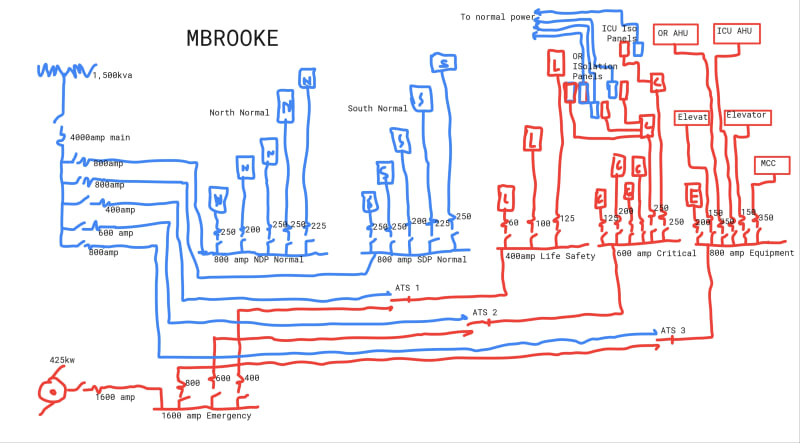
In summary, the total amount of emergency power for most buildings (and therefore the amount of emergency distribution equipment needed) is typically 10% or less and consists of only that minimal amount of power needed to help people safely exit a building within the first few minutes of normal power interruption. For hospitals, emergency power becomes the life blood of a building without utility power and must be maintained throughout a power outage, which could last for days after a storm or other catastrophic event. As a result, it’s not unusual to see the emergency power of a hospital exceed 50% or 60% of the building’s total power needs. Also, as separate transfer switches are need for each type of load (life safety, critical, nondelayed automatic equipment, delayed automatic equipment, and delayed automatic or manual connection equipment loads), multiple ATSs are always needed for hospitals. For a 200,000-sq-ft hospital, eight or more transfer switches could be used. A similarly sized office building would typically have only two ATSs.